Before a revolutionary smart insulin pump can transform a patient’s life, it must pass a critical test of its safety plan. Developing the technology is only half the battle for medical innovators. According to federal law, you cannot legally ship an unapproved, high-risk medical prototype across state lines for human trials without a specific green light from the government. For connected or wearable devices, factor in fda cybersecurity guidelines for medical devices and recent us fda guidelines that may shape your test strategy under broader regulatory guidelines.
Securing this permission requires an Investigational Device Exemption, widely known as an IDE. Think of this document as a restricted driver’s license for a new invention, proving your technology is clinically ready and safe for testing on patients. Proper IDE planning and submission acts as your legal exemption from standard marketing rules, ensuring your upcoming trial aligns perfectly with FDA guidelines.
Once your comprehensive safety package leaves the office, a highly anticipated countdown begins. In practice, regulators operate on a strict 30-day review clock to evaluate your safety evidence. This one-month window stands as the most important timeline for your project, determining whether your clinical trial can finally begin or if your team must head back to the drawing board.
Is Your Device ‘Significant Risk’? How to Tell Before the FDA Does
Before you can test a new invention on humans, you must answer a critical question: how dangerous could this be if something goes wrong? To establish safety paths, the FDA categorizes testing into Significant Risk vs Non-Significant Risk devices. This distinction determines whether you need a massive regulatory submission or a simplified path to start your study.
A product is high-risk if it is implanted, sustains life, or could cause serious harm if it fails. To see the difference under current regulatory guidelines, compare these common examples:
- Significant Risk: Surgical lasers, implanted pacemakers, and artificial heart valves.
- Non-Significant Risk: Daily step-counters, external wound dressings, and standard athletic joint braces.
You cannot simply declare your own invention safe. Every study requires an Institutional Review Board (IRB), an independent committee at a hospital or clinic dedicated to protecting patients. You must present a clearly documented case to this committee justifying your risk level. Securing IRB approval for clinical investigations as a low-risk product often lets you skip the formal FDA application and begin testing immediately.
Misjudging this classification can halt your research for months while you scramble to gather more data. When the line between high and low risk is blurry, guessing is an expensive mistake. Fortunately, there is a way to get early feedback on your strategy, which is why the FDA Pre-Submission Meeting is your secret weapon for approval.
Why the FDA Pre-Submission Meeting is Your Secret Weapon for Approval
Guessing what regulators want is a quick way to get your research paused. Instead of risking a “clinical hold” a strict order stopping your trial over unexpected safety concerns smart developers use a Q-Submission. This serves as a free consultation before taking a final exam. A strong FDA pre-submission meeting strategy uncovers hidden requirements and aligns your testing methods long before the official paperwork is due.
Timing is crucial; request this meeting three to six months before your IDE. An experienced pharma regulatory compliance solution provider will emphasize that while FDA feedback here is “non-binding” (meaning they can adapt if new risks emerge), it establishes vital regulatory and informational markers for your journey. To ensure success, structure your presentation to secure clear “yes” or “no” answers rather than vague opinions. In practice, regulatory and informational markers are identified through which features of your protocol endpoints, enrollment criteria, monitoring plans, and risk mitigations so make each element explicit and testable.
Securing agreement on your strategy dramatically reduces your chances of a devastating disapproval. When stepping into that discussion, always bring these four essential questions:
- Do you agree with our proposed risk classification?
- Is our patient sample size large enough to prove safety?
- Does our patient selection criteria match your expectations?
- Are our proposed testing endpoints acceptable?
With clear feedback in hand, you are ready for the next step: Packing the Regulatory Suitcase: The Must-Have Files for Your IDE Application.
Packing the Regulatory Suitcase: The Must-Have Files for Your IDE Application
Securing permission to test high-risk devices means proving you are fully prepared. The official rulebook for this is Part 812, and achieving FDA 21 CFR Part 812 compliance simply means satisfying those foundational safety rules. Preparing your application is akin to packing a regulatory suitcase; before regulators approve your clinical journey, they must inspect specific folders to ensure you are ready for the trip. Plan for formatting and traceability early, aligning with ectd guidelines fda where applicable, and cross-referencing broader regulatory guidelines.
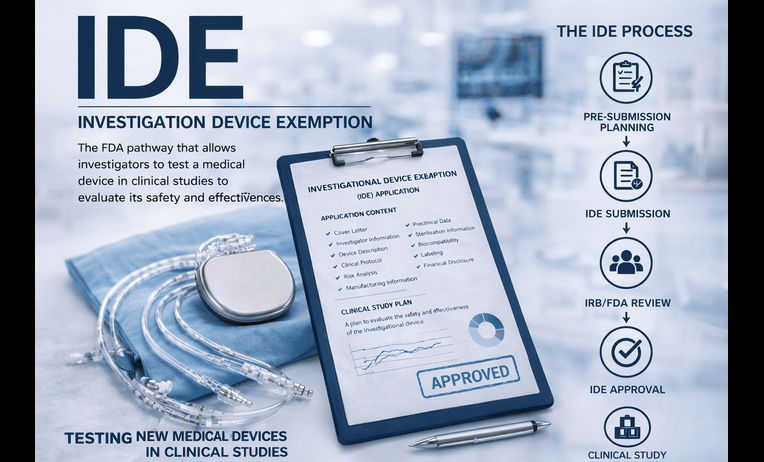
Meeting Investigational device exemption regulatory requirements means carefully packing these five core folders into your submission:
- Device Description: How the invention physically functions.
- Manufacturing Details: Proof of consistent, safe assembly.
- Investigator Agreements: Signed contracts with your testing doctors.
- Report of Prior Investigations: Your historical safety data.
- Investigational Plan: Your exact roadmap for the human study.
Align manufacturing and testing artifacts with good manufacturing practices guidelines and guidelines for environmental monitoring; where assays are involved, follow method validation guidelines, method validation guidelines ich, and analytical method validation ich guidelines. Many teams also lean on validated electronic batch record solutions providers to keep builds consistent and traceable. If your dossier will later transition to marketing submissions, track format and content early against ectd guidelines fda and related regulatory guidelines. Consult ich guidelines for quality concepts that may overlap with device expectations; if your team is new to these frameworks and wonders what is ich guidelines, start with the ICH Q-series for grounding.
Regulators will scrutinize your Report of Prior Investigations more than anything else in that suitcase. This file holds all preclinical data like lab bench tests or animal studies justifying the leap to human subjects. If you built a new surgical laser, this report proves it cuts tissue without causing unintended burns, confirming the potential medical benefits heavily outweigh the risks. If you work with sterile handling environments, the usp 797 guidelines 2023 (and the broader usp 797 guidelines) can inform expectations for cleanroom practices and documentation rigor, even when your primary pathway is device-focused.
Your Investigational Plan acts as the step-by-step manual for the doctors conducting the test. Mastering how to write a clinical trial protocol is crucial here, as this specific document strictly dictates patient treatment and safety monitoring criteria. Once your regulatory suitcase is packed, you must decide what kind of testing journey to take. This choice leads directly to Early Feasibility vs. Pivotal Studies: Choosing the Right Trial for Your Goal.
Early Feasibility vs. Pivotal Studies: Choosing the Right Trial for Your Goal
Before launching a massive medical trial, you must decide what exactly you need to prove. If your invention is brand new and still evolving, you might start with an Early Feasibility Study (EFS). Consider this a limited “test drive.” At this stage, your medical device pilot study objectives focus heavily on tweaking the design and gathering initial safety data rather than proving universal effectiveness.
Once your design is locked, you need a rigorous test to earn final FDA permission. This is the Pivotal Study, which relies on strict “trial endpoints” specific, measurable goals like a twenty percent drop in a patient’s blood pressure. When comparing a pivotal study vs feasibility study, remember these three core differences:
- Size: Feasibility involves a handful of patients; pivotal requires hundreds.
- Goal: Feasibility refines prototypes; pivotal proves the final product is safe and effective.
- Outcome: Feasibility leads to better designs; pivotal generates the exact data needed for market approval.
As you finalize endpoints and power calculations, ask up front: what does a confidence interval represent in your context? Choose standard confidence interval notation and anticipate the confidence interval range needed to show acceptable performance. Understand prediction vs confidence interval, prediction interval and confidence interval trade-offs, and when to apply a tolerance interval vs confidence interval during design verification and validation. Selecting the right test dictates your overall roadmap. For instance, distinguishing the de novo pathway vs IDE clarifies that an IDE grants permission to test on humans, while De Novo is your eventual legal path to sell a novel device. Submitting vague endpoints will instantly stall your progress, leading directly to a dreaded scenario: Avoiding the ‘Clinical Hold’: Why Most IDE Applications Fail and How to Fix Them.
Avoiding the ‘Clinical Hold’: Why Most IDE Applications Fail and How to Fix Them
Submitting your application kicks off a strict thirty-day countdown. By law, the agency has exactly one month to review your safety plans. If day thirty-one arrives and you have heard absolutely nothing, you legally have a green light to start testing. This unique regulatory quirk is called “passive approval,” acting as an automatic permission slip for well-prepared applicants.
However, perfect silence from reviewers is rare. You will typically receive one of three official responses: a full Approval, an Approval with Conditions allowing you to start while fixing minor gaps, or a Disapproval. Understanding the common reasons for IDE disapproval—like glaring safety risks or missing testing details—is crucial for your timeline. When an application hits a serious roadblock, the FDA issues a deficiency letter outlining the exact problems. This formal rejection triggers a legal freeze on your trial.
Bouncing back requires systematically resolving FDA clinical hold issues rather than arguing with the reviewers. You must provide the missing proof of safety, often relying on oos fda guidelines (Out of Specification) to explain any unexpected early test results from your prototype phase. If your device includes connectivity, be ready to map mitigations to fda cybersecurity guidelines for medical devices and any recent us fda guidelines touching your risk profile; when appropriate, provide patient-facing materials consistent with fda med guides to support safe use. Once you satisfy the agency’s demands and earn that final approval letter, the real work begins. Your focus must immediately shift toward executing the trial properly, which transitions seamlessly into Managing Life After Submission: Data Integrity and Clinical Compliance.
Managing Life After Submission: Data Integrity and Clinical Compliance
Earning the FDA’s green light is a major milestone, but your trial’s success depends entirely on what happens next. Every piece of information your device generates must be bulletproof to survive future inspections. This ongoing commitment is governed by gxp guidelines a broad set of quality standards ensuring your study runs safely and legally. GxP acts as the overarching rulebook guaranteeing your final results are actually trustworthy.
Regulators enforce this rulebook using strict data integrity guidelines in pharma and medical devices. The gold standard for this is the alcoa guidelines, a simple framework ensuring every patient record is reliable:
- Attributable: Who recorded the data?
- Legible: Is the information easy to read and permanent?
- Contemporaneous: Was it recorded exactly when it happened?
- Original: Is this the source document, not a copy?
- Accurate: Is it perfectly correct and error-free?
Managing this overwhelming detail shouldn’t fall solely on your shoulders. Many companies use a functional service provider model to share the workload. Depending on scope, this may include functional service providers for data management, eTMF providers, eCOA providers, and a provider clinical support system to support sites. If you are running studies in the EU, partnering with a european scientific service provider can streamline country-specific requirements. Keep chain-of-custody tight by aligning with pharmaceutical logistics providers compliance. The functional service providers market is broad and also intersects with pharmacovigilance solution providers for post-market surveillance, letting you focus fully on Your Roadmap to a Successful IDE Submission and Beyond.
Regulatory landscapes evolve quickly—policy shifts like the eu ban titanium dioxide e171 food additive 2022 regulation (often summarized as the eu ban titanium dioxide food additive 2022 regulation) highlight the titanium dioxide ban in Europe and illustrate how fast requirements can change. Maintain a proactive horizon scan.
Your Roadmap to a Successful IDE Submission and Beyond
You now have the tools to navigate the regulatory maze with confidence. Instead of seeing the FDA as a roadblock, you can approach them as a partner in patient safety. You understand the journey from assessing your device for Significant Risk to packing your data “suitcase,” and you know exactly how long is the FDA IDE review period (just 30 days).
To keep your momentum, follow this 5-step checklist for your next 90 days of IDE planning and submission:
- Determine your device’s exact risk level.
- Organize your initial prototype safety data.
- Identify a hospital review board (IRB) for your study.
- Draft a clear summary of your clinical test plan.
- Request a pre-submission meeting with the FDA.
These rules exist to protect patients, but they do not have to halt your innovation. If the legal steps feel overwhelming, consider partnering with a regulatory compliance expert to streamline your strategy. Shortlist the best life sciences technology solutions providers in USA or specialized qms consulting services riverside california to fill gaps, and engage functional partners early. Start your pre-submission planning today—doing the right groundwork now prevents months of costly delays later.
Q&A
Question: What is an Investigational Device Exemption (IDE) and why do I need it before human testing?
Short answer: An IDE is the FDA’s permission to clinically test a high‑risk, unapproved device in humans. It functions like a restricted driver’s license legally exempting you from standard marketing rules so you can ship and use a significant‑risk prototype across state lines. By submitting an IDE, you assert that your device is clinically ready and sufficiently safe for patient testing. Once filed, the FDA operates on a strict 30‑day review clock that determines whether your trial can start, proceed with conditions, or be halted for more data.
Question: How do I determine whether my device is Significant Risk (SR) or Non‑Significant Risk (NSR), and who makes the call?
Short answer: SR devices are implanted, sustain life, or could cause serious harm if they fail (e.g., surgical lasers, implanted pacemakers, artificial heart valves). NSR examples include step‑counters, external wound dressings, and standard joint braces. You cannot self‑declare; an Institutional Review Board (IRB) reviews your rationale and approves the classification. If the IRB agrees your study is NSR, you can often begin without a formal FDA IDE. Misclassification can cause long delays, so when the line is blurry, use an FDA Pre‑Submission (Q‑Submission) to get early, non‑binding feedback. Go in with focused, yes/no questions on risk classification, sample size, selection criteria, and endpoints.
Question: What are the must‑have components of a strong IDE submission?
Short answer: Pack five core “folders” that align with FDA 21 CFR Part 812:
- Device Description (how it works)
- Manufacturing Details (evidence of consistent, safe assembly)
- Investigator Agreements (signed commitments from study clinicians)
- Report of Prior Investigations (all preclinical and historical safety data)
- Investigational Plan (your clinical protocol: endpoints, enrollment, monitoring, mitigations)
Plan formatting/traceability early per ectd guidelines fda. Align with good manufacturing practices guidelines and guidelines for environmental monitoring; where assays apply, follow method validation guidelines, method validation guidelines ich, and analytical method validation ich guidelines. For sterile environments, consult usp 797 guidelines 2023. For connected/wearable devices, map risks and mitigations to fda cybersecurity guidelines for medical devices and recent us fda guidelines. Many teams use validated electronic batch record solutions providers to keep builds consistent and traceable.
Question: Should I run an Early Feasibility Study (EFS) or jump to a Pivotal Study?
Short answer: Choose EFS when your design is still evolving and you need limited, early safety and usability insights; choose a Pivotal Study once the design is locked and you must rigorously prove safety and effectiveness for marketing. Key differences:
- Size: EFS = a handful of patients; Pivotal = hundreds.
- Goal: EFS refines prototypes; Pivotal confirms final safety/effectiveness via predefined endpoints.
- Outcome: EFS improves design; Pivotal generates approval‑ready evidence.
Define clear, measurable endpoints and plan statistics up front know what a confidence interval represents in your context, choose standard notation, and decide when to use confidence vs prediction vs tolerance intervals during verification/validation. Remember: IDE permits human testing; the de novo pathway vs IDE distinction is that De Novo is a later route to market authorization for novel devices.
Question: What happens during the FDA’s 30‑day IDE review, and how do I avoid or recover from a clinical hold?
Short answer: After submission, the FDA has 30 days to respond. Outcomes are typically Approval, Approval with Conditions (you may start while addressing minor gaps), or Disapproval. If day 31 arrives with no feedback, you may proceed under “passive approval.” Disapprovals come with a deficiency letter effectively a clinical hold detailing what to fix. To recover, provide the missing safety evidence, address unexpected results using oos fda guidelines as appropriate, and, for connected devices, map mitigations to fda cybersecurity guidelines for medical devices along with any recent us fda guidelines; supply patient materials consistent with fda med guides when relevant. After approval, protect your study’s credibility through gxp guidelines and the alcoa guidelines (Attributable, Legible, Contemporaneous, Original, Accurate). Many teams leverage a functional service provider model (e.g., data management, eTMF, eCOA, site support) and maintain compliant logistics; if running in the EU, a european scientific service provider can help with local requirements. Keep a proactive horizon scan, as regulations evolve quickly.